Author: Lung and Esophageal Cancer Multidisciplinary Team, Dr. Chih-Hsun Shih
Dr. Chih-Hsun Shih, a distinguished senior physician in the Thoracic Surgery Department at KFSYSCC, specializes in surgical interventions for lung cancer, esophageal cancer, mediastinal tumors, and diverse types of lung metastatic cancers. Dr. Shin holds a Bachelor's degree in Medicine from National Yangming University and a Master's degree in Clinical Medicine from China Medical University. He has been part of KFSYSCC since 2005, following a stint as a lecturer for the Ministry of Education in 2004. His previous roles also include being an assistant professor in the Department of Medicine at National Yang Ming University and supervisor at the Taiwan Thoracic and Cardiovascular Surgery Medical Association. Currently, he is a crucial member of the multidisciplinary integrated diagnosis and treatment team for lung and esophageal cancer at our hospital.
Patients Treated at KFSYSCC Can Feel Reassured
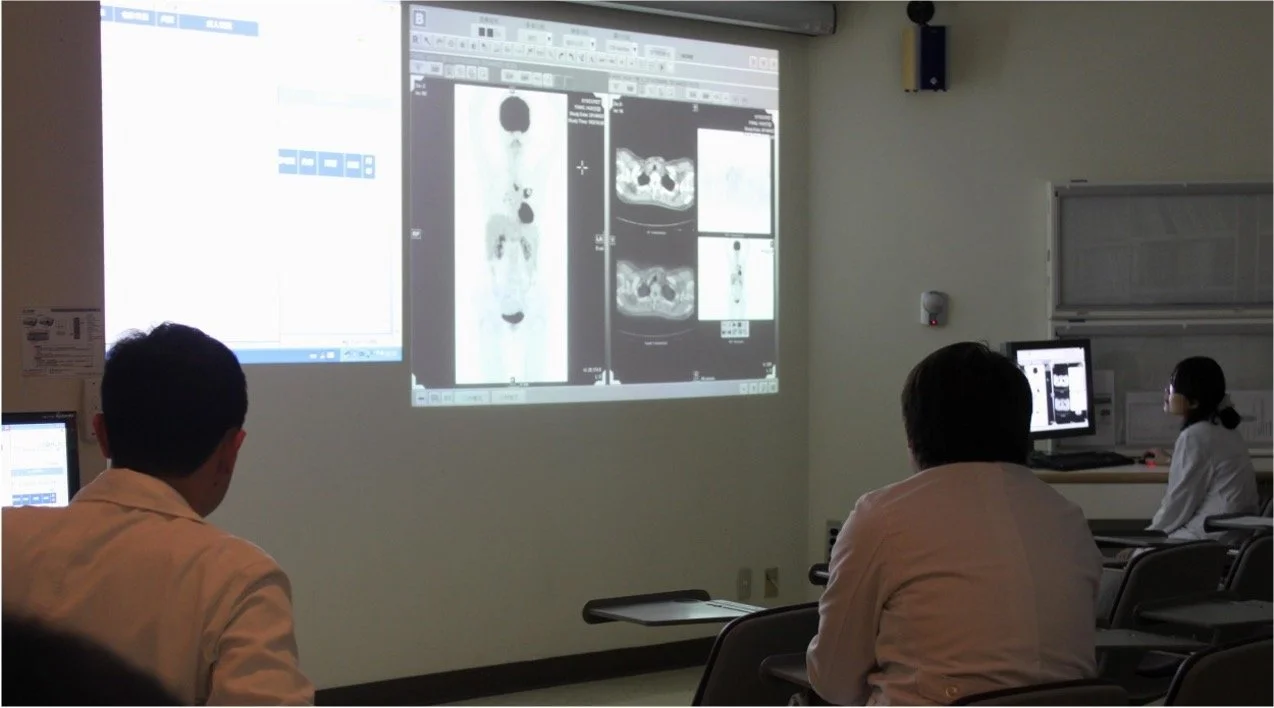
Observing our lung cancer team's operational mechanisms and the unwavering commitment of our medical staff in patient care underlines the collaboration between patients and an extensive team of healthcare professionals in a nurturing and empathetic environment.
Established in 1990, KFSYSCC is a beacon for cancer care in Taipei, surrounded by various other medical centers as the first specialized cancer hospital in Taiwan. As we enter our third decade, we continue to pioneer local clinical oncology with our unwavering dedication and rigorous approach.
Preserving our mission has been a significant challenge. Today, KFSYSCC stands as the sole specialized cancer hospital in Taiwan. Reflecting on its foundation, when Dr. Andrew T. Huang, a Duke University Medical Center alumnus, dedicated himself entirely to the planning and establishment of the hospital. He meticulously attended to every detail, from the hospital's architectural layout to the organization of the medical team, patient safety and privacy, and the creation of a comforting medical environment. Furthermore, he fostered an environment of humanistic care, mutual trust, and understanding, embedding these principles in every facet of the hospital's operations and daily medical activities.
Before joining KFSYSCC, I spent years honing my skills at various public and private medical centers. Initially, I was drawn to KFSYSCC due to its unique workplace culture. After over a decade working here, I deeply resonate with and am ingrained in KFSYSCC’s organizational ethos.
Emphasized by President/CEO Dr. Huang in his book ”Doing Right," the structure of our medical team is critical. He firmly believes that only a well-coordinated medical team can offer patients the most comprehensive services. Accordingly, since our hospital's inception, there has been a significant focus on multidisciplinary teams. We trust that the consensus developed through these team meetings provides superior cancer treatment compared to the outdated approach of relying on individual leading physicians.
Concerning the operation of our hospital's multidisciplinary cancer treatment team, while it adheres to professional treatment guidelines and considers multiple aspects, its core principle is prioritizing the patient's best interests. As Dr. Huang remarked, "The hospital exists for the patients, and all considerations should be patient-centered." To illustrate this, I'd like to share the case of a late-stage lung adenocarcinoma patient who sought treatment at our hospital, highlighting the functionality of our lung cancer treatment team.
Ms. Lin, a 65-year-old retired civil servant, was informed of an abnormality in her chest x-ray during a routine health check. Subsequent investigation confirmed lung adenocarcinoma. Her tumor, over six centimeters in diameter, was suspected of having metastasized to the mediastinal lymph nodes. She was diagnosed with locally advanced stage III lung cancer, or potentially stage IVa with pleural metastasis.
At this stage of lung adenocarcinoma, immediate surgical removal isn't typically recommended due to the complexities and potential complications. Therefore, a customized treatment plan is critical, and neoadjuvant therapy can be considered to reduce tumor size and increase the chances of complete surgical removal.
Our multidisciplinary integrated treatment approach is based on improving the overall cure rate and long-term survival rate of lung adenocarcinoma. Even with advancements in targeted therapies and immune therapies, without the potential for surgery, the treatment efficacy is limited. Therefore, our approach involves considering neoadjuvant chemotherapy, targeted therapy, or even immunotherapy to control or shrink the lung tumor, reduce the overall number of cancer cells, lower metastasis risk, and increase the chances of complete malignant tumor cell resection.
Given the current understanding of lung adenocarcinoma management, initiating surgical intervention at advanced stages (III or IV) is often discouraged. There exists a lack of consensus regarding the optimal approach to treatment planning, necessitating patient-specific strategies. An early surgical approach to excise the tumor might initially appear proactive and reasonable, aimed at eliminating malignancy and better delineating the disease's scope. Following surgery, subsequent therapies, including adjuvant chemotherapy or radiation, are usually guided by pathological findings. However, this approach might pose potential pitfalls if the cancer has metastasized or is not completely resectable, causing undue organ damage and possibly delaying overall treatment.
A plausible alternative could be neoadjuvant therapy, administered before the principal treatment, to circumvent potential surgical inefficacy.
Emerging evidence from recent clinical studies and international expert reviews suggests that the success of surgical tumor resection significantly impacts the cure rates and long-term survival of lung adenocarcinoma patients. Despite advancements in chemotherapeutic agents and the introduction of targeted therapies and immunotherapies, treatment options remain constrained if surgery is not a viable option and patients must rely solely on pharmacotherapy or radiation therapy. Therefore, neoadjuvant chemotherapy, targeted therapy, or even immunotherapy is being explored to control or reduce tumor size, minimize the total cancer cell volume, curtail metastasis chances, and improve the likelihood of complete surgical resection. Following surgery, additional treatment may be indicated to prevent local recurrence. Generally, the decision to post-operatively administer adjuvant radiochemotherapy, targeted therapy, or immunotherapy is guided by the pathological report, contributing to comprehensive disease control. This encapsulates the principle and practice of multi-disciplinary integrated treatment.
Faced with the daunting task of making treatment decisions, Mrs. Lin and her family consulted various medical centers in Taiwan, receiving a wide array of professional advice. Suggestions ranged from enrolling in clinical trials to explore novel immunotherapies to initiating immediate surgery. In Taiwan, the main specialties involved in diagnosing and managing lung adenocarcinoma include pulmonology, thoracic surgery, and hematology-oncology, leading to a diversity of opinions that left the family feeling overwhelmed and uncertain.
Despite her son being a seasoned clinician, deciphering a vast array of specialist information in a brief period—including clinical trial data, surgical techniques, and newly published treatment protocols—was a significant challenge, making rational and appropriate clinical decisions difficult to formulate.
In their distressed state, the Lin family turned to the pulmonology department at KFSYSCC for an initial consultation. Despite their confusion about managing Mrs. Lin's lung adenocarcinoma, multiple consultations at various centers had equipped them with extensive knowledge about her disease, including diagnostic imaging, biopsy findings, whole-body tumor staging, and recommended treatment strategies.
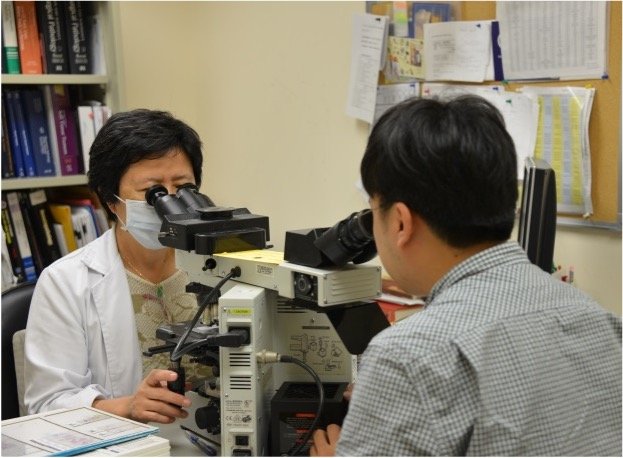
During the initial consultation, the attending physician verified Mrs. Lin's medical records, conducted a focused physical examination, and elaborated on our standard operating procedures for patients with previous diagnoses or treatments from other hospitals. Prior to initiating any treatment, we require a pathology slide re-interpretation to confirm the cancer diagnosis. While this process demands time, it helps ensure patient safety by minimizing the risk of misinterpretation and inappropriate treatment unless there's an urgent clinical situation. Our lead clinician will liaise with the clinician from the original hospital and proceed with treatment only after obtaining the patient's and family's understanding and consent, following thorough documentation of the patient’s condition.
We also re-interpret any imaging studies performed at other hospitals and perform thorough cardio-pulmonary and physiological assessments to ensure no aspect of patient care is overlooked. To facilitate communication and coordination, we assign a case manager specializing in lung cancer to accompany the patient throughout the treatment process and subsequent outpatient follow-ups.
A week after her primary consultation, Mrs. Lin and her family from Taiwan’s southern region, revisited KFSYSCC under the guidance of her assigned care nurse. Scheduled meetings were in place with her oncologist and thoracic surgeon. In advance of these consultations, both specialists were briefed on her health status during a lung cancer team meeting at the hospital. The radiologist and nuclear medicine physician had analyzed and shared imaging results, providing the staging for Mrs. Lin's lung adenocarcinoma. Following this, the thoracic surgeon reviewed her cardio-pulmonary evaluation findings and potential surgical risks.
The medical team then deliberated on the optimal treatment pathway, considering KFSYSCC’s lung cancer treatment protocol, as well as global oncology society recommendations. Factors such as the patient's age, physiological capabilities, tumor stage, genetic mutation profile, and the extent of tumor spread were evaluated. The team proposed targeted therapy as the initial approach for Mrs. Lin's lung adenocarcinoma, given her positive Epidermal Growth Factor Receptor (EGFR) mutation status and a stage IIIA or IVA diagnosis. This treatment would serve as a neoadjuvant therapy, closely monitored for tumor regression, typical adverse reactions like certain rashes and diarrhea caused by the oral therapy, as well as symptoms potentially arising from tumor lysis syndrome.
Oral targeted therapy is becoming preferred over traditional chemotherapy due to its ease of administration, no hospitalization requirement, quick response, and lesser side effects. However, a crucial criterion is a positive EGFR status in the lung adenocarcinoma, a requirement for receiving National Health Insurance reimbursement. The positive result also predicts higher chances of tumor regression. This trend signifies a notable evolution in oncology due to the significant strides in molecular biotechnology and genetic analysis, leading to more personalized and tailored treatments.
Within a month of targeted drug administration, Mrs. Lin experienced visible tumor reduction, the sole side effect being skin papules. She was thoroughly briefed on her treatment plan, making her experience less intimidating than initially feared. The care coordinator, well-versed in lung cancer, addressed all her queries with compassion and knowledge. Mrs. Lin found comfort in having a reliable point of contact, which eased her daily life. She looked forward to her consultations with the medical team, in addition to maintaining a healthy diet and routine activities.
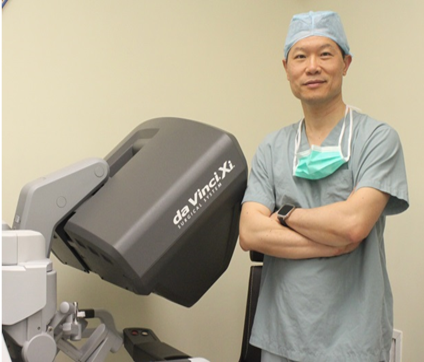
After the targeted therapy, a sequence of imaging tests including chest CT scans, brain MRIs, and a full-body PET scan was scheduled for tumor assessment. Comparisons of these new images with previous ones revealed her lung adenocarcinoma's reduction to about three centimeters with no discernible growth in the surrounding lymph nodes. The lung cancer team agreed on proceeding with the surgical resection through single-port thoracoscopic surgery, planning to remove the right lower lobe and associated lymph nodes.
KFSYSCC’s Department of Thoracic Surgery was a pioneer in Taiwan for thoracoscopic minimally invasive surgery, which has evolved to single-port surgery. Almost 90% of lung surgeries at our hospital are performed via a single port, achieving the goal of minimally invasive surgery while reducing surgical time, material costs, post-operative pain, and recovery time.
Mrs. Lin underwent a successful single-port thoracoscopic surgery on the right side. An intraoperative examination of the pleura, interlobar surfaces, and relevant anatomical locations was conducted. Suspicious regions were biopsied for further analysis, and the tumor's extent was precisely determined to assess the need for adjuvant therapy. The surgery successfully concluded, with no unexpected findings of tumor spread. Her recovery was rapid, and she reported no need for pain medication at her one-week postop consultation.
In advanced lung cancer management, if neoadjuvant therapy effectively reduces the tumor size followed by appropriate surgical resection, the postoperative pathological findings become crucial in deciding the need for radiotherapy. These results also provide an estimate of the patient's risk of recurrence or metastasis. In Mrs. Lin's case, we adopted a sequence of targeted therapy leading to significant tumor reduction, followed by curative surgery. This approach enhances the probability of total surgical resection, averting potential issues of incomplete resection and residual tumor, had surgery been the initial step.
Indeed, initiating neoadjuvant therapy before surgery requires careful consideration of several uncertain factors. These include potential side effects of the chosen therapeutic drugs. If the chosen regimen fails to sufficiently shrink the tumor to meet the set objectives, it may hamper subsequent surgical interventions, or potentially foster the growth of an exceptionally malignant tumor, which might eventually prevent the opportunity for surgical intervention.
The entire treatment protocol necessitates a multi-disciplinary approach and close coordination among various specialists. The crux of successful implementation lies in an integrated multi-disciplinary consensus and its thorough application. Our lung cancer treatment team typically starts with solid groundwork for complex cases. This involves meticulously compiling, interpreting, and reorganizing each patient's clinical data. This allows a comprehensive review of all relevant factors during collective team discussions.
Moreover, we value feedback from frontline healthcare providers and case managers and take into account the patient's individual preferences. This approach ensures adherence to the professional ethics of competence and promoting justice. We require every team member to contribute their expertise towards formulating a personalized treatment plan for each patient.
The real-world outcomes and feedback from clinical treatments are invaluable for the team's continuous growth and improvement. For example, in the case of Mrs. Lin, who successfully adhered to the treatment plan proposed by our team, we reported the results back to the team in a timely manner and included them in follow-up records. This process not only enriches the team's collective clinical experience but also fosters an environment of continual self-improvement, which is essential to maintain the team's dynamism and growth.
Turning back to Mrs. Lin's case, a thorough surgical examination allowed for the complete removal of the tumor since it had not spread locally. Pathological examination confirmed the absence of any residual tumor at the surgical margins, and all excised lymph nodes were free of cancer cells. This represented an ideal surgical outcome with complete tumor eradication. However, initial radiological imaging suggested that the tumor was exerting pressure on surrounding organs. This necessitates collective discussion within the team to decide whether additional adjuvant chemotherapy, radiation therapy, or the continuation of the successful targeted therapy is needed.
Drawing from past experiences within our lung cancer team, we deliberated on Mrs. Lin's initial diagnosis, the original treatment plan, intraoperative findings, pathological results, and current literature, along with expert opinions from various clinical departments. The result was a recommendation for adjuvant chemotherapy post-surgery. In the interest of patient's quality of life and economic considerations, we temporarily decided against the continued use of targeted therapy.
This narrative exemplifies the typical process undertaken by our lung cancer team in dealing with complex cases of lung adenocarcinoma. Our philosophy, as often emphasized by Dean Huang, is to maintain a keen focus on details and to constantly be receptive to patient feedback.
Observing the practical operations of our lung cancer team, it becomes clear that our clinical treatments are underscored by commitment and a deep sense of care. We believe that as one gains insight into our team operations, it is evident that our patients, within a warm and human-centric environment, are collaboratively battling tumors alongside our dedicated medical team. It's comforting to note that our patients are indeed in good hands and can feel confident about their treatment journey at our hospital.