
Interview with Dr. Rong-Long Chen, Pediatric Cancer Multidisciplinary Team: The Key to Curing Metastatic, Relapsed Germ-Cell Tumors with Triple-Tandem Transplantation
At age twenty-three, “Ah-Chih” (a pseudonym) was diagnosed at a southern medical center with a mediastinal germ-cell tumor, a highly aggressive cancer. He followed the standard plan: surgical removal of the mass, chemotherapy, and even prophylactic radiation. Within a single year his tumor markers surged again. Surgeons suspected a local relapse and operated, but pathology found no cancer cells. Two months later new symptoms appeared. One side of his tongue swelled, speech became difficult, tinnitus troubled his left ear, severe pain struck the left occipital region, and his eye felt uncomfortably full. Detailed imaging revealed a skull-base tumor. It was metastatic, relapsed germ-cell cancer originating from the mediastinum.
Some cases few are willing to take on still appear in clinic despite remarkable progress against germ-cell tumors. The American Society of Clinical Oncology has highlighted this disease group as one of its landmark advances, with cure rates now dramatically improved. Testicular cancer in particular reaches cure in about 95 percent of cases. Yet a small subset remains difficult to diagnose and treat, and Ah-Chih fell into that category.
On the recommendation of a KFSYSCC patient, he traveled north to Koo Foundation Sun Yat-Sen Cancer Center and sought care from Dr. Rong-Long Chen, who convenes the pediatric cancer multidisciplinary team. Dr. Chen graduated from National Taiwan University College of Medicine. In 1995 he conducted cell-therapy research, including gene transfer and immunotherapy, at Children’s Hospital Los Angeles. In 1997 he presented work on immune activation in neuroblastoma at the American Association for Cancer Research annual meeting and received a Young Investigator Award. Over more than forty years of practice, he has specialized in pediatric hematology-oncology and hematopoietic stem-cell transplantation and is widely respected in the field.
Dr. Chen recalls that, according to data from advanced centers at the time, relapsed cases like Ah-Chih’s had only a 4 percent rescue rate without high-dose transplantation. A single high-dose transplant raised that figure to about 10 percent, and even those few initial successes lacked long-term survivors. Given KFSYSCC’s strong collaboration with leading international teams, the clinicians decided to try a different path. They adopted the triple-tandem transplantation strategy reported by Dr. Darren Feldman at Memorial Sloan Kettering Cancer Center, giving Ah-Chih one last chance.
KFSYSCC became the first hospital in Taiwan to attempt triple-tandem transplantation for metastatic, relapsed germ-cell tumors. Dr. Chen convened a meeting with the patient and his family, explained the scientific rationale and potential impacts in detail, and proposed the rescue plan. Encouraged by relatives and friends, Ah-Chih agreed. He completed treatment, overcame the disease, and has remained free of recurrence for more than ten years, which amounts to a complete recovery.
Building on this success, KFSYSCC subsequently treated three additional patients with relapsed mediastinal primary germ-cell tumors using the same approach and cured two of them.
An Innovative Therapy Brings New Hope
Triple-tandem transplantation combines chemotherapy with stem-cell rescue for metastatic or treatment-resistant malignant germ-cell tumors. In brief, high-dose chemotherapy is used to eliminate cancer cells, but it also damages normal cells, including the bone marrow. After tumor burden is driven down, hematopoietic stem-cell transplantation is performed to rebuild marrow function and restore blood-cell production. This cycle is repeated three times within two months so that malignant cells die before they can replicate. The goal is to reduce the cancer to a level the immune system can handle, achieving cure.
Germ-cell tumors cover a wide range. Common types include teratoma; yolk sac tumor, which often appears in children; dysgerminoma in the ovary; and seminoma in the testis. These are sometimes grouped under the umbrella of “germinomas” or germ-cell tumors. Rarer entities include embryonal carcinoma, choriocarcinoma, and gonadoblastoma. Choriocarcinoma is especially dangerous. It spreads through blood vessels, destroys tissue and organs, and can trigger massive hemorrhage.
Dr. Chen emphasizes that not every germ-cell tumor requires triple-tandem transplantation. Mature teratomas or tumors without other metastases can often be cured with surgery, with chemotherapy considered as needed. When radiation is necessary, it is usually for germinomas or tumors located in the brain. In other words, standard therapy is effective for most patients. Only a small group like Ah-Chih’s demands a triple-tandem approach.
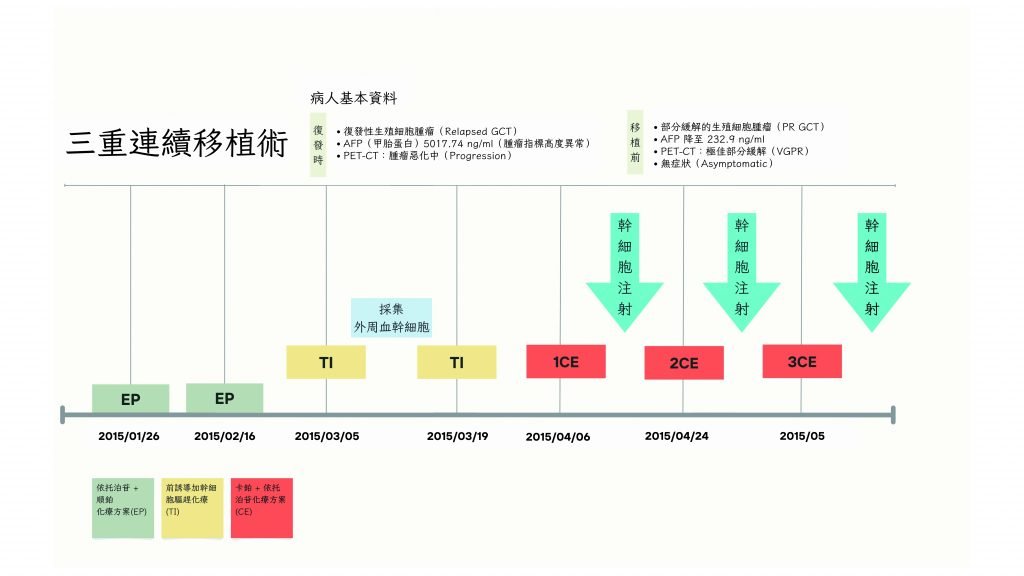
A treatment chart illustrates a young woman with metastatic yolk sac tumor whose alpha-fetoprotein (AFP) levels fell sharply after EP and TI regimens. PET-CT then showed an excellent partial response. That response, combined with the subsequent antitumor effect of high-dose CE, increased the likelihood that stem-cell transplantation would succeed.
Multidisciplinary Integration Raises the Odds of Success
Triple-tandem transplantation carries real risk and does not suit everyone. Dr. Chen explains that, beyond whether a patient can tolerate powerful drugs, the tumor must be highly sensitive to chemotherapy, and an adequate number of stem cells must be collected beforehand. Although this therapy has been used for more than a decade in advanced countries, few hospitals in Taiwan have attempted it, including some large medical centers.
Why could KFSYSCC do it and achieve a success rate above 60 percent? Dr. Chen points to strict adherence to safety standards and a detailed plan that safeguards each step. Since 2012 the hospital has built a treatment platform centered on hematopoietic stem-cell transplantation. It has successfully rescued many patients referred for difficult leukemias, neurologic diseases, and tumors, and the same integrated strengths shine when triple-tandem therapy is used for germ-cell tumors.
He adds that KFSYSCC’s integrated model proves its worth throughout the process. Team members from nursing, nutrition, infection control, pharmacy, pathology, neurology, respiratory therapy, intensive care, endocrinology, rehabilitation, psychosocial care, and surgery each play a careful, specific role. Before treatment, clinical pharmacists establish pharmacokinetic monitoring so drug levels remain therapeutic without tipping into toxicity. To secure a higher yield of stem cells, social workers obtain assistance for costly next-generation mobilizing agents. Because infection is the major concern during therapy, the multidisciplinary team operates a comprehensive prevention protocol to keep patients safe.
To date, ten complex cases have undergone triple-tandem transplantation at KFSYSCC. Five are very likely cured, and one more recently completed treatment and is under follow-up. The program is both feasible and effective. Although KFSYSCC does not run a pediatric outpatient clinic, many germ-cell tumor patients arrive as high-risk referrals from other hospitals. “Another challenging case is coming next week,” Dr. Chen notes, a patient who relapsed after second-line therapy. With success rates exceeding 60 percent, triple-tandem transplantation offers new hope and may benefit many more patients.
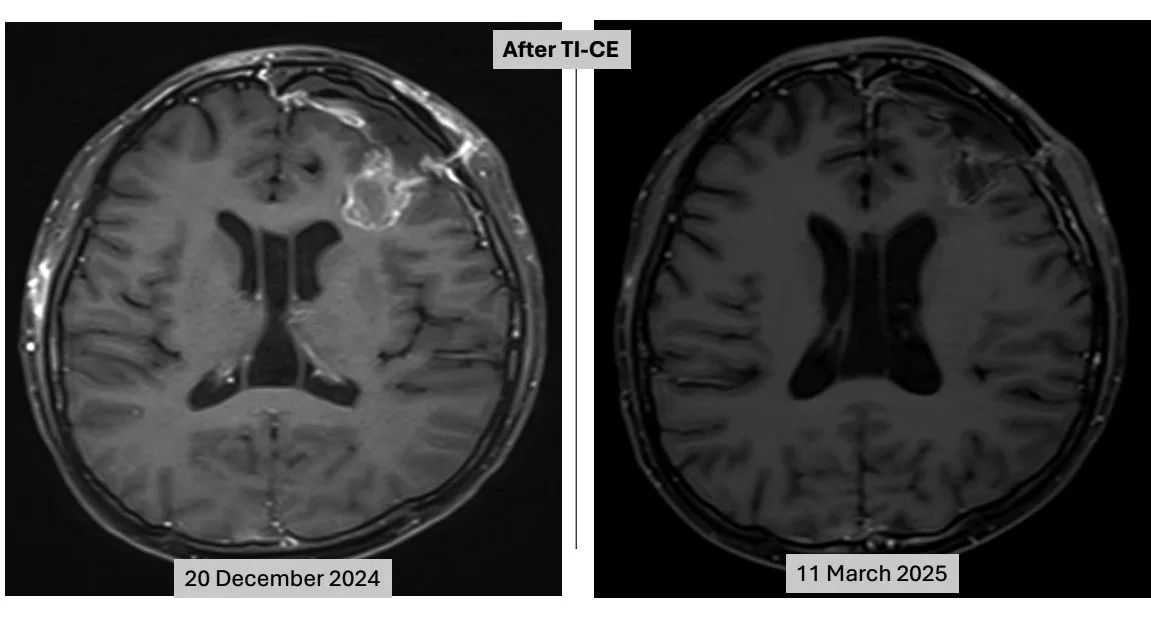
After triple-tandem transplantation, imaging showed a pronounced treatment response at the site of the brain metastasis. Before therapy (left image): a rim-enhancing, hyperintense mass was visible in the subcortical region of the left cerebral hemisphere (which appears on the right side of the image). After therapy (right image): the lesion in the same area had almost completely disappeared, with only minor post-treatment changes—such as scarring or a small fluid space—and no clear residual disease, indicating an excellent response.
Questions Patients Ask Most
Q: What is a germ-cell tumor?
A: Germ-cell tumors arise when primordial germ cells become malignant in the gonads or outside them. During embryonic development these cells should migrate from the yolk sac and mesentery to the pelvis or scrotum to form the ovaries or testes. If development goes awry, some cells may settle elsewhere and transform, producing tumors not only in the gonads but also in the central nervous system, sacrococcygeal region, mediastinum, retroperitoneum, and other sites.
Q: At what ages do germ-cell tumors occur, and what symptoms are common?
A: They can occur at any age, with peaks before age five and again during adolescence. Symptoms vary by location. Testicular tumors often present as a painless scrotal mass. In women, ovarian teratomas are most common and may cause pain, nausea, or vomiting. In infants, sacrococcygeal tumors often protrude visibly after birth. Central nervous system tumors can cause nausea, vomiting, or blurred vision. Mediastinal tumors may compress the airway and lead to cough, shortness of breath, or chest pain.
Q: Can children be treated with triple-tandem transplantation?
A: Children are generally very sensitive to chemotherapy. Most can be treated successfully with surgery and appropriately tailored chemotherapy. Only a small group with high-risk relapse requires triple-tandem therapy.
Q: What side effects should patients expect?
A: High-dose chemotherapy can cause discomfort such as nausea and hair loss. Based on KFSYSCC’s clinical observations, the most troublesome problems often relate to mucositis and its complications, including infection, sore throat, and abdominal bloating. These effects are usually short-lived and tend to ease once treatment ends.